Rationing Medications During Shortages: How Ethical Decisions Are Made
 Mar, 24 2026
Mar, 24 2026
When a life-saving drug runs out, who gets it? This isn’t a hypothetical question-it’s happening right now in hospitals across the U.S. In 2023, the FDA recorded 319 active drug shortages, with critical cancer drugs like carboplatin and cisplatin in short supply for months. Oncologists faced impossible choices: give a dose to one patient with stage IV ovarian cancer, or another with the same prognosis. No one wants to play God. But when supply breaks down, someone has to decide-and those decisions need to be ethical, not random.
Why Medication Rationing Is Happening Now
Drug shortages aren’t new, but they’ve gotten worse. In 2005, there were 61 shortages. By 2011, that number jumped to 251. Today, it’s over 300. The main culprits? A fragile supply chain, too few manufacturers, and reliance on overseas production. Just three companies make 85% of generic injectable drugs in the U.S. When one factory shuts down for quality issues, entire drug classes vanish overnight. Sterile injectables-like chemo drugs, antibiotics, and anesthetics-are the most vulnerable. They’re hard to make, hard to store, and hard to replace.The Ethical Frameworks That Guide Decisions
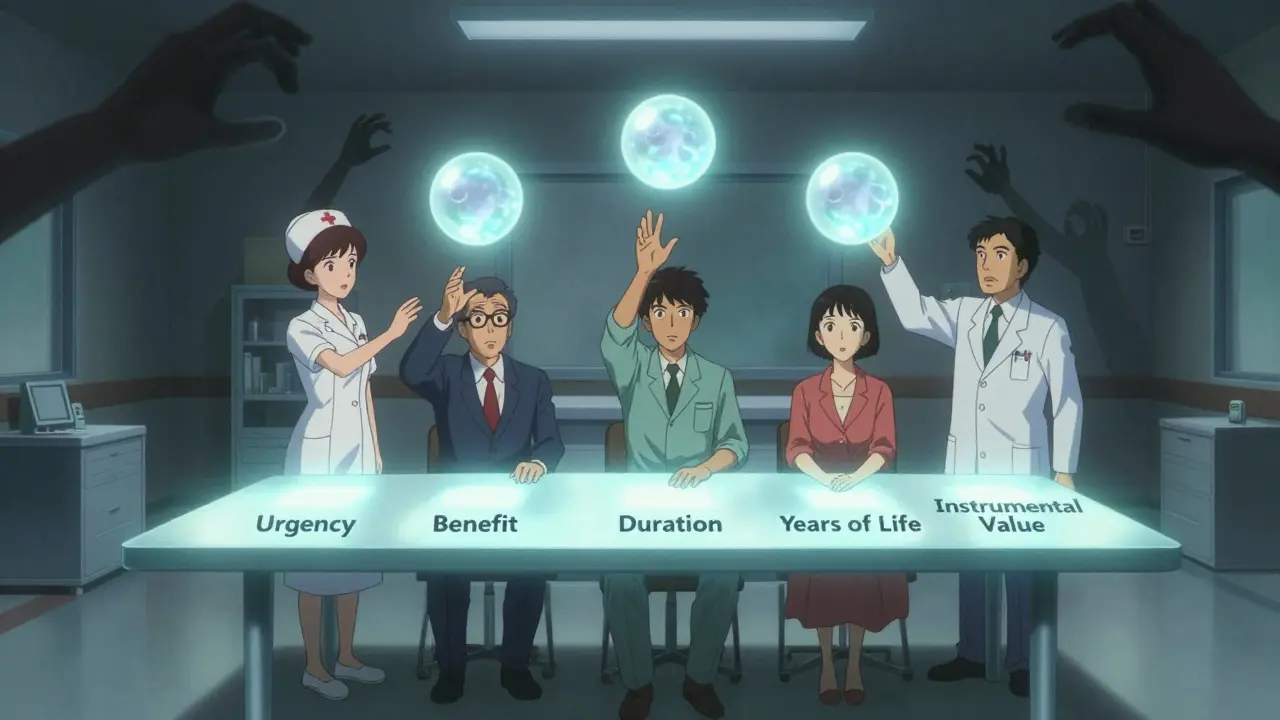
Ethical rationing isn’t about guessing or flipping a coin. It’s built on clear, evidence-based principles. The most widely accepted model comes from Daniels and Sabin’s "accountability for reasonableness" framework. It requires four things: publicity (everyone knows how decisions are made), relevance (criteria must be grounded in medical evidence), appeals (patients or families can challenge a decision), and enforcement (someone makes sure rules are followed). The American Society of Clinical Oncology (ASCO) added cancer-specific rules in 2023. Their guidance says allocation should happen at the committee level-not at the bedside. A team of pharmacists, oncologists, nurses, ethicists, and even patient advocates should review cases. This isn’t bureaucracy-it’s fairness. Bedside decisions, made under pressure, lead to bias, inconsistency, and burnout. Five core criteria are used to rank patients:- Urgency of need-Who will die without this drug?
- likelihood of benefit-Is there a real chance this treatment will work?
- duration of benefit-Will it extend life for weeks, months, or years?
- Saving the most years of life-Prioritizing younger patients with longer life expectancy
- Instrumental value-Do they serve a critical function (e.g., frontline healthcare workers)?
What Happens When There’s No System?
In many hospitals, there’s no formal process. A 2022 study in JAMA Internal Medicine found that over half (51.8%) of rationing decisions were made by individual clinicians alone. That’s not ethics-it’s survival mode. Nurses and doctors are left to choose between patients with no guidance. The result? Higher burnout, moral distress, and deep inequities. One oncologist shared on ASCO’s forum: "I’ve had to choose between two stage IV ovarian cancer patients for limited carboplatin doses three times this month with no institutional guidance." That’s not a rare story. Only 4.9% of hospital committees include ethicists. Only 13.3% include physicians. That’s not a team-it’s a gap. Rural hospitals are hit hardest. Sixty-eight percent have no formal rationing protocol. Urban academic centers? Only 32% lack one. That means a patient in Nebraska might get a lifesaving drug because their hospital has a committee, while someone in a nearby town gets nothing. The system isn’t broken-it’s uneven.How Hospitals Are Trying to Fix This
Some places are doing better. The Minnesota Department of Health released a detailed plan in April 2023 for carboplatin and cisplatin shortages. It ranked patients into tiers:- Tier 1: Curative intent, no alternative therapy available
- Tier 2: Palliative intent, but treatment significantly improves quality of life
- Tier 3: Alternative therapies exist
Jefferson Moratin
March 25, 2026 AT 01:58The ethical frameworks outlined here are rigorously sound, but they rest on a foundational assumption: that medical resources can be objectively quantified. In reality, utility metrics like 'years of life saved' implicitly devalue the elderly, the disabled, and those with comorbidities. This isn't neutrality-it's utilitarianism disguised as fairness. We must ask: who defines 'benefit'? Is a 72-year-old with metastatic cancer less worthy of dignity than a 35-year-old with the same prognosis? The answer reveals more about our cultural biases than our clinical protocols.
Moreover, the reliance on institutional committees ignores the moral agency of clinicians. Doctors aren't cogs in a machine. They're trained to make life-or-death judgments. Removing their discretion under the banner of 'fairness' risks creating a bureaucratic hellscape where patients become data points, not people.
Transparency is non-negotiable. If a patient isn't told their treatment is rationed, the entire system collapses into moral hypocrisy. Trust isn't just a byproduct-it's the foundation. Without it, even the most 'ethical' algorithm becomes a tool of oppression.
Caroline Dennis
March 25, 2026 AT 19:35ASCO’s tiered allocation model is the bare minimum we should be implementing nationwide. Urgency + likelihood of benefit + duration of benefit-these aren't arbitrary. They're evidence-based. The real failure isn't the framework-it's the lack of enforcement. Hospitals without ethicists on committees are functionally operating in a legal gray zone. And let’s be clear: when a nurse has to choose between two stage IV patients, that's not triage-it's trauma.
We need federal mandates. Not suggestions. Mandates. With audits. With penalties. This isn't philosophy. It's public health infrastructure. And we're failing at the most basic level.
Zola Parker
March 26, 2026 AT 11:44So we’re prioritizing young people over old ones now? 😒
What’s next? Euthanizing the unproductive? 🤡
At least back in the day, we just gave meds to whoever screamed loudest. 😅
florence matthews
March 28, 2026 AT 02:33I’m from Canada, and honestly? We’ve had rationing for decades. Not because we’re better, but because we had to be. Our system doesn’t pretend to be perfect-it just tries to be fair. No one gets left behind because they can’t afford a private hospital. Maybe the U.S. needs to stop treating healthcare like a marketplace and start treating it like a right.
Also-thank you for mentioning transparency. That’s the part no one talks about. Patients deserve to know why they’re being denied. It’s not cruel to tell them. It’s cruel to lie by silence. 🫶
Kenneth Jones
March 28, 2026 AT 18:45Raphael Schwartz
March 30, 2026 AT 11:53USA bad. China makes all the drugs. Why we let them?
WE NEED TO MAKE DRUGS HERE.
NO MORE FOREIGN DRUGS.
MAKE AMERICA GREAT AGAIN.
TRUMP WAS RIGHT.
WE WERE WINNING.
WE ARE WINNING.
WE WILL WIN AGAIN.
STOP THE STEAL.
DRUGS ARE OURS.
NO MORE SHORTAGES.
JUST MAKE THEM.
Marissa Staples
March 31, 2026 AT 14:31I think the real issue isn’t who gets the drug-it’s why we’re running out in the first place. We’ve outsourced production to save a few cents per pill. Now we’re paying with lives. That’s not a medical crisis. That’s a corporate crime. And no algorithm fixes that.
Fix the supply chain. Then worry about who gets what.
Grace Kusta Nasralla
April 1, 2026 AT 11:56I just… I can’t. I work in oncology. I’ve had to tell people their treatment is on hold. I’ve seen the look in their eyes. Not anger. Not sadness. Just… emptiness.
And then I go home and cry in the shower.
And no one asks me how I’m doing.
They just want the next decision.
How do you live with that?
Korn Deno
April 2, 2026 AT 02:14Let’s not romanticize committees. They’re slow. They’re bureaucratic. They’re full of people who’ve never held a dying patient’s hand. But they’re also the only thing standing between chaos and collapse.
The alternative? A nurse choosing between two women with stage IV ovarian cancer because her boss told her to. That’s not ethics. That’s a nightmare.
Yes, the system’s flawed. But we don’t throw out the rulebook because the game’s rigged. We fix the rules. And we hold people accountable.
And yes-patients deserve to know. No exceptions.
Stephen Alabi
April 3, 2026 AT 00:29One must interrogate the underlying epistemological assumptions of the Daniels-Sabin framework. It presumes that medical decision-making can be rationalized through procedural justice, yet it fails to account for ontological uncertainty inherent in clinical practice. The very notion of 'likelihood of benefit' is statistically ill-posed when applied to individual patients with heterogeneous disease trajectories.
Furthermore, the reliance on 'years of life saved' as a metric is a reductio ad absurdum of utilitarianism. It implicitly assigns differential moral worth based on age and prognosis-a form of institutionalized ageism masquerading as clinical objectivity.
One must ask: if a 70-year-old patient has a 60% chance of survival, and a 25-year-old has a 55% chance, is the former less deserving? Or is the metric itself the injustice?
Perhaps the solution is not allocation-but redistribution of manufacturing capacity. Or perhaps, more radically, we must abandon the notion of scarcity entirely and treat healthcare as a public good.
Until then, we are merely tending to the symptoms of a diseased system.
Pat Fur
April 4, 2026 AT 04:49My mom had ovarian cancer. She got her carboplatin because her hospital had a committee. She’s still here. Five years later.
But her best friend? Same stage. Same age. Same everything. Her hospital didn’t have a policy. She got nothing.
I don’t care how fair your algorithm is. If two people with the same diagnosis get different fates because of where they live… that’s not a system. That’s a lottery.
And we’re betting lives on it.
Linda Foster
April 5, 2026 AT 04:24It is imperative that institutional protocols be standardized, transparent, and ethically grounded. The absence of formalized decision-making structures constitutes a systemic failure of governance in healthcare delivery. One cannot rely on ad hoc clinical judgment in matters of life and death. The evidence presented herein underscores the necessity of policy implementation at the federal level. Without regulatory oversight, equity remains aspirational rather than operational.
Caroline Bonner
April 7, 2026 AT 03:42I just want to say how deeply moved I am by this post. Seriously. This isn’t just about drugs or shortages-it’s about what kind of society we want to be. Do we value people based on how long they can live? Or do we value them because they’re human? I work in hospice care, and I’ve seen people who were told they had six months live for five years… and others who got the drug and still left us in three weeks. There’s no predicting it. No spreadsheet can capture that.
And what about the families? The ones who don’t even know their loved one was on a waiting list? That’s not just a policy gap-that’s a soul wound. I’ve held hands with mothers who whispered, ‘I don’t understand why they stopped.’ And I had to lie and say, ‘It’s just how it is.’
Let’s stop pretending we’re making hard choices. Let’s start demanding better systems. Let’s fund the committees. Let’s train the ethicists. Let’s tell the truth. Even if it hurts. Even if it’s messy. Even if it’s inconvenient.
Because people are worth it.
And we owe them more than a spreadsheet.
Chris Crosson
April 8, 2026 AT 21:11One thing no one talks about: what happens when a patient appeals? Who even handles that? In most hospitals, there’s no process. No form. No person. Just silence. And that silence? It’s the loudest part of this whole crisis.
We need a national hotline. A dedicated team. A live person who answers when someone says, ‘Why did they give it to her and not me?’
It’s not rocket science. It’s basic decency.